Table of Contents
-
1. Quick Answer
-
2. Overview
-
3. What Is a Diabetic Foot Ulcer?
-
4. How Is a Diabetic Foot Ulcer Diagnosed?
-
5. Treatment for Diabetic Foot Ulcer
-
5.4 Infection Control
-
5.5 Revascularisation
-
5.6 Blood Sugar Management
-
5.7 Additional Therapies
6. How to Prevent Diabetic Foot Ulcers?
7. Take Home Message
8. FAQs
Quick Answer
- Diabetic Foot Ulcer Treatment Goal: Heal the wound, control infection and prevent amputation
- Core Approach: Wound debridement, strict offloading, and blood sugar control
- Infection Control: Antibiotics targeted to severity and wound culture: oral for mild, IV for deeper infections
- Circulation Support: Revascularisation improves blood flow in ischaemic ulcers, which is essential for healing
- Advanced Care: NPWT, specialised dressings and surgery for wounds that don’t respond to standard care
Overview
Diabetic foot ulcer treatment focuses on healing the wound, controlling infection and improving circulation to prevent complications. Management involves pressure offloading, wound debridement, antibiotics and revascularisation.
Complex or non-healing ulcers require advanced wound care and vascular interventions, which are best managed by vascular surgeons in collaboration with a foot specialist or podiatrist.
Early diagnosis, consistent care and blood sugar control help improve outcomes and reduce the risk of amputation.
What Is a Diabetic Foot Ulcer?
A diabetic foot ulcer is an open wound that develops due to a combination of nerve damage, prolonged pressure and poor blood circulation. These ulcers commonly occur on weight-bearing areas such as the sole, heel or toes.
Loss of sensation delays detection of minor injuries, while impaired healing in diabetes allows wounds to persist and progress into chronic, non-healing ulcers.
How Is a Diabetic Foot Ulcer Diagnosed?
Most diabetic foot ulcers are detected late because nerve damage eliminates the pain that would normally prompt attention. Here are two important signs that can help diagnose a diabetic foot ulcer at home:
- Skin temperature: a warm spot on one part of the foot compared to another can indicate active inflammation or infection; coolness suggests poor circulation. Patients can check this at home by feeling both feet with the back of the hand
- Skin and nail inspection: peeling, cracking, maceration between toes, thickened nails, and colour changes are early warning signs. Patients can and should do this daily
Once these early warning signs are identified, a detailed clinical evaluation helps confirm the diagnosis and determine the severity of the ulcer.
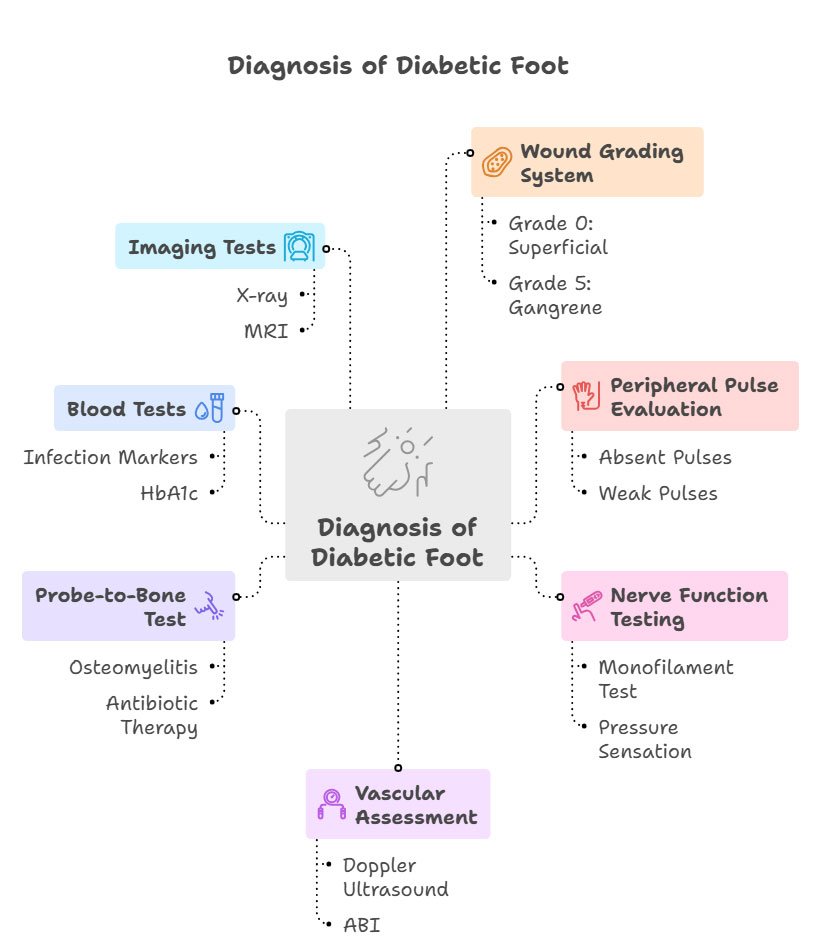
- Wound grading system (Meggitt-Wagner classification) stages the diabetic foot ulcer from grade 0 for a superficial wound to 5 for gangrene: the grade determines how aggressively treatment needs to begin
- Peripheral pulse evaluation: pulses at the ankle and foot are felt by hand; absent or weak pulses signal poor arterial flow and risk of delayed healing
- Nerve function testing using a monofilament checks if you can feel pressure on your foot: if you can’t, you may have been walking on an injury for days without knowing it
- Vascular assessment using Doppler ultrasound and ABI measures circulation to the foot: an ischaemic ulcer without adequate blood supply will not heal, regardless of other treatment
- Probe-to-bone test checks whether infection has reached the bone: osteomyelitis requires prolonged antibiotic therapy or surgery, and changes the entire treatment plan
- Blood tests to assess infection markers and HbA1c: uncontrolled blood sugar at the time of diagnosis is one of the strongest predictors of poor healing
- X-ray or MRI is advised when deep infection, bone damage, or gas in tissues is suspected; it detects complications not visible on the surface
These findings determine whether the ulcer is neuropathic, ischaemic, or neuroischaemic, and the type determines the treatment approach.
Diabetic foot ulcer treatment focuses on four key pillars: offloading, wound debridement, infection control and restoring blood flow, along with effective blood sugar control to support healing.
Treatment for Diabetic Foot Ulcer
Offloading Techniques
Unrelieved pressure prevents healing in diabetic foot ulcers, and offloading redistributes the load away from affected areas.
- Offloading prevents repeated trauma and allows wound healing
- Types of offloading footwear: Non-removable total contact casts (TCC) are the gold standard; other options are removable cast walkers and half shoes for patients who cannot tolerate a TCC
- Offloading should continue after healing is complete to prevent recurrence
At the CIIVES department, custom insoles and offloading footwear are provided as part of the treatment plan at our Diabetic Foot Care Clinic (DFCC).

Wound Debridement
Dead tissue and callus can delay healing and require debridement to prepare the wound for repair.
- Removal of dead tissue, infected material and surrounding callus to reduce bacterial load
- Promotes the formation of healthy granulation tissue and prepares the wound bed
- Regular debridement improves the effectiveness of dressings and overall healing outcomes
Debridement may be performed surgically, enzymatically, or through autolytic methods using specialised dressings, depending on wound severity and circulation status.
Wound Management
Effective wound care focuses on maintaining a clean, moist environment that supports tissue healing and prevents complications.
- Moisture-retentive dressings (hydrogels, alginates, foam) protect the wound and maintain a healing environment
- Negative-pressure wound therapy (NPWT) applies controlled suction to remove excess fluid and reduce swelling
- Surgical interventions include abscess drainage, infected tissue removal and reconstructive procedures
Infection Control
Infection can rapidly worsen a diabetic foot ulcer. It spreads to deeper tissues, reaches the bone, and can trigger gangrene, making early treatment critical.
- Antibiotics are selected based on infection severity and culture results if available
- Mild infections are managed with oral therapy, while deeper infections may require intravenous antibiotics
- Early treatment prevents spread to deeper tissues and bone infection or osteomyelitis
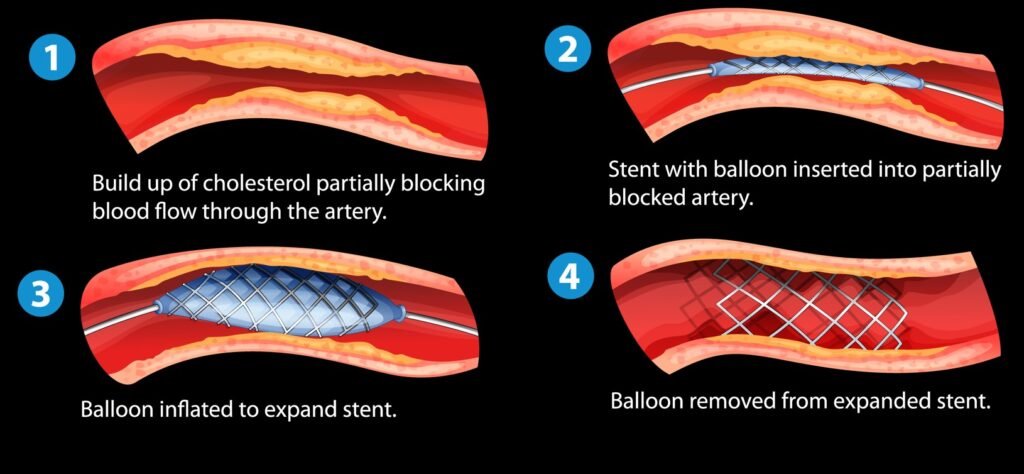
Revascularisation
Poor blood flow limits healing, so restoring circulation is essential in patients with ischaemic ulcers.
- Procedures such as peripheral angioplasty or bypass surgery restore blood flow
- Improves oxygen and nutrient delivery, which is critical for healing ischaemic ulcers
- Often required in patients with peripheral arterial disease (PAD)
Revascularisation for diabetic foot and critical limb ischaemia should ideally be performed by a qualified vascular surgeon. They are best equipped to manage complex cases through both endovascular procedures and open surgery, ensuring successful outcomes.
Blood Sugar Management
Glycaemic control runs parallel to all wound care; uncontrolled blood sugar:
- Impairs immune response
- Delays healing
- Creates an environment favourable for bacterial growth
- Significantly increases recurrence risk
Additional Therapies
Some complex or non-healing ulcers may require supportive therapies to enhance healing.
- Hyperbaric oxygen therapy (HBOT) – delivering high-concentration oxygen under pressure to improve tissue oxygenation
- Used as an adjunct therapy in selected non-healing or ischaemic ulcers that have not responded to conventional treatment
How to Prevent Diabetic Foot Ulcers?
Prevention of diabetic foot ulcers involves early detection and reducing pressure or injury to the feet.
- Inspect feet daily for cuts, blisters or skin changes
- Wear properly fitted footwear to avoid pressure points and friction
- Maintain foot hygiene and moisturise to prevent cracks
- Control blood sugar levels to support tissue health
- Avoid walking barefoot to reduce the risk of unnoticed injuries
- Schedule regular medical check-ups to monitor nerve function and circulation


At the CIIVES Department, Dr Preeti Gupta leads Nagpur’s only Diabetic Foot Care Clinic (DFCC), offering regular foot screening and monitoring for high-risk diabetic patients. Early review can prevent a minor concern from becoming a major complication.
Take Home Message
Diabetic foot ulcers begin with minor, unnoticed changes, but delayed treatment leads to serious complications. What makes them challenging is the combination of nerve damage, poor circulation and impaired healing. Daily self-checks, early reporting of small changes in drainage or temperature, and consistent follow-up can greatly improve treatment outcomes.
Long-term prevention is as important as treatment, due to high recurrence rates without continued care. Recognising risk early and acting promptly is one of the most effective ways to protect foot health and avoid avoidable complications.
FAQs
How To Heal a Diabetic Foot Ulcer Naturally?
Diabetic foot ulcers do not heal effectively with home remedies alone and require medical care. Basic measures such as keeping the wound clean, protected and pressure-free can support healing.
Blood sugar control and proper nutrition also play an important role. Delayed or improper treatment increases the risk of infection, deeper tissue damage and complications.
What Are the Early Signs That a Diabetic Foot Ulcer Is Healing?
Healing ulcers show a gradual reduction in size and depth, along with the formation of healthy pink or red tissue. Drainage, swelling and redness decrease.
Moreover, there are no signs of infection, such as foul odour or pus. Over time, the wound edges begin to close, indicating recovery and tissue repair.
When Is Surgery Required for Diabetic Foot Ulcers?
Surgery is considered when there is deep infection, abscess formation or bone involvement (osteomyelitis). It may also be required if the ulcer does not respond to medical treatment or if there is tissue death or gangrene.
In patients with poor circulation, revascularisation procedures may be needed to restore blood flow and support healing.