
Quick Answer
- AAA Treatment Goal: Prevent aneurysm rupture, control growth and reduce the risk of fatal internal bleeding
- When Aneurysm Repair is Needed: AAA repair is generally advised once the aneurysm reaches 5.0-5.5 cm, becomes symptomatic or expands rapidly
- AAA Treatment Options: Endovascular aneurysm repair (EVAR) and open surgical repair (OSR)
- Ruptured AAA: Sudden rupture causes severe abdominal or back pain with internal bleeding and requires emergency vascular surgery
- Recovery & Follow-Up: Lifelong imaging surveillance is important after AAA repair to detect graft-related complications or recurrent aneurysm expansion
Synopsis
Modern abdominal aortic aneurysm treatment includes identifying risk factors to regularly monitor susceptible populations. For small aneurysms, a wait-and-watch strategy is preferred, and for large or symptomatic aneurysms, surgical repair is advised.
Endovascular aneurysm repair (EVAR) offers a minimally invasive option with faster recovery, while open surgical repair (OSR) remains essential for complex aneurysm anatomy and ruptured cases.
Early diagnosis and timely vascular intervention are critical to improving survival and preventing rupture.
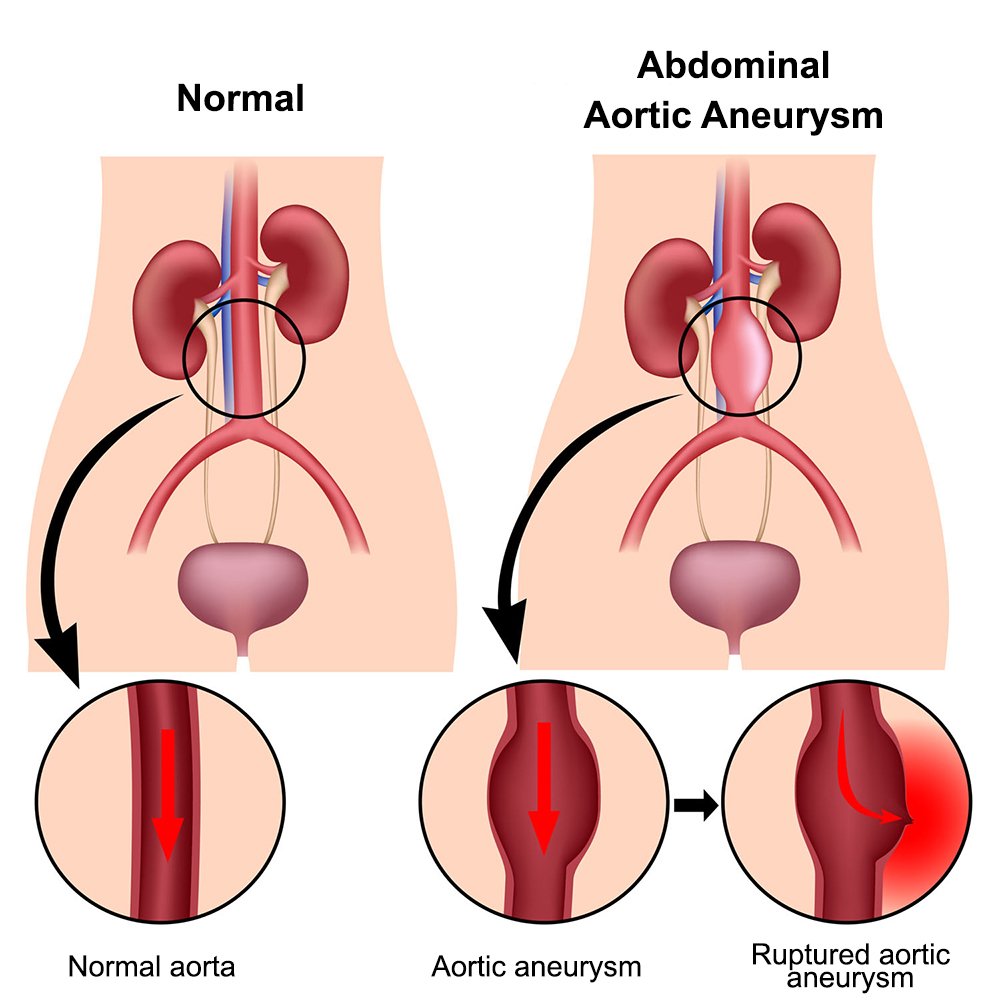
What Is an Abdominal Aortic Aneurysm?
An abdominal aortic aneurysm (AAA) is an irreversible, localised enlargement of the abdominal aorta, most commonly occurring below the level of the kidneys due to weakening of the vessel wall. An aneurysm is generally defined when the aortic diameter enlarges to at least >1.5× the normal diameter.
Most AAAs develop silently over time and may not cause symptoms until they enlarge significantly. As the aneurysm expands, wall tension increases and so does the risk of rupture. Studies show that aneurysms larger than 5.5 cm carry a substantially higher risk of rupture, making early detection and treatment extremely important.
What Are Ruptured Aneurysms (rAAA)?
A ruptured abdominal aortic aneurysm occurs when the weakened aortic wall is torn, causing sudden and severe internal bleeding. Common symptoms of AAA rupture include intense abdominal or back pain, dizziness, collapse and low blood pressure.
Ruptured AAA is a life-threatening vascular emergency with extremely high mortality if not treated immediately. Emergency EVAR or open surgical repair may be performed depending on the patient’s condition, bleeding severity and aneurysm anatomy.
How Is an Abdominal Aortic Aneurysm Diagnosed?
Most AAAs are discovered incidentally during scans performed for unrelated symptoms. In many cases, abdominal discomfort or back pain is initially mistaken for digestive or muscular problems before imaging reveals the aneurysm.
Once an aneurysm is suspected, a detailed vascular evaluation helps determine its size, rupture risk and need for treatment.
- Abdominal ultrasound: First-line screening tool used to detect and monitor AAA size due to its accuracy, speed and non-invasive nature
- CT angiography (CTA): Provides detailed information about aneurysm anatomy, leakage, rupture risk and suitability for EVAR or surgery
- Physical examination: A pulsatile abdominal mass may be felt during examination, especially in leaner patients
- Aneurysm growth monitoring: Expansion greater than 0.5 cm within 6 months indicates increased rupture risk and may require intervention
- Screening in high-risk individuals: Recommended in older smokers, patients with hypertension or those with a family history of aneurysm disease
- Assessment for associated aneurysms: Imaging may also identify peripheral aneurysms, such as popliteal or femoral aneurysms, which can coexist with AAA
These findings help vascular surgeons determine whether regular surveillance or surgical repair is the safest treatment approach.
Abdominal Aortic Aneurysm Treatment
AAA treatment depends on aneurysm size, symptoms, expansion rate and overall rupture risk.
Small aneurysms are usually monitored with regular imaging, while symptomatic, rapidly enlarging or large aneurysms often require surgical repair to prevent rupture.
Treatment planning also includes optimising blood pressure, smoking cessation, and cardiovascular risk reduction to improve long-term outcome
Monitoring & Conservative Management of AAA
Small or stable aneurysms may not require immediate surgery but need careful surveillance to reduce rupture risk.
- Regular imaging surveillance: Ultrasound or CT scans monitor aneurysm size and expansion rate over time
- Blood pressure control: Reduces mechanical stress on the weakened aortic wall
- Smoking cessation: Slows aneurysm progression and lowers surgical risk
- Cholesterol management: Helps control associated atherosclerotic disease
- Exercise and lifestyle modification: Supports long-term vascular health
- Surgical threshold monitoring: Repair is recommended once aneurysm diameter reaches ≥5.5 cm in men and ≥5.0 cm in women, as women have a higher rupture risk at smaller aneurysm sizes
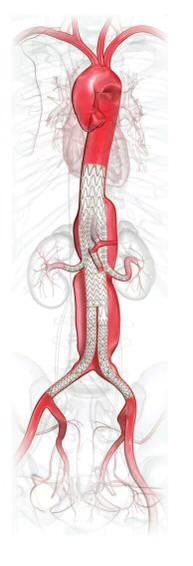
Endovascular Repair of AAA
- Minimally invasive procedure using a stent graft inserted through the femoral artery
- Diverts blood flow away from the aneurysm sac to reduce rupture risk
- Associated with shorter hospital stay and faster recovery than open surgery
- Requires long-term imaging surveillance to detect endoleaks or graft complications
Preparing for AAA Surgery
Before aneurysm repair, patients undergo evaluation to assess surgical fitness and reduce complications.
- Cardiac and vascular assessment: Evaluates heart health and operative risk
- CT angiography planning: Helps determine suitability for EVAR or open repair
- Blood investigations: Assess kidney function, clotting status and overall fitness
- Medication review: Blood thinners or certain drugs may require adjustment before surgery
- Smoking cessation before surgery: Improves healing and reduces respiratory complications
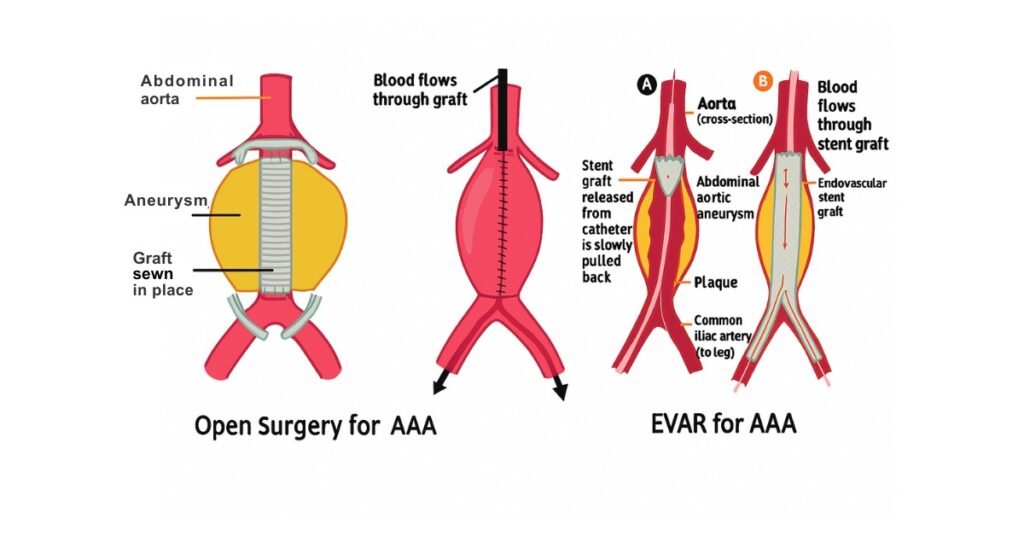
Endovascular Aneurysm Repair (EVAR)
EVAR is a minimally invasive abdominal aortic aneurysm repair procedure performed through small groin incisions using a stent graft.
- Procedure: A stent graft is inserted through the femoral artery and positioned inside the aneurysm to redirect blood flow
- How it works: Reduces pressure on the aneurysm wall and lowers rupture risk without removing the aneurysm sac
- Best suited for: Older patients, high-risk surgical candidates and anatomically suitable aneurysms
- Advantages: Smaller incisions, shorter hospital stay, faster recovery and reduced blood loss
- Recovery timeline: Most patients recover within 3-6 weeks with a gradual return to daily activities
- Long-term follow-up: Lifelong imaging surveillance is required to detect endoleaks, graft migration or recurrent aneurysm expansion
- Limitation: Not suitable for all aneurysm anatomies, especially complex neck anatomy or severe vessel tortuosity
In some cases, EVAR may need to be converted to open surgery during the same procedure due to anatomical or technical challenges.
Complex aneurysms near the kidney or intestinal arteries may also require advanced techniques such as fenestrated EVAR (FEVAR), branched EVAR (BEVAR), or chimney EVAR (Ch-EVAR) to maintain blood flow to vital organs while safely sealing the aneurysm.
Open Surgical Repair (OSR)
Open surgical repair involves direct replacement of the aneurysmal segment with a synthetic graft through a major abdominal operation.
- Procedure: The weakened aortic segment is clamped, opened and replaced with a synthetic graft
- Best suited for: Complex aneurysm anatomy, connective tissue disorders or patients unsuitable for EVAR
- Durability: Provides excellent long-term repair with lower reintervention rates
- Hospital stay: Usually longer than EVAR, often around 5-10 days, depending on recovery
- Recovery timeline: Full recovery may take 2-3 months
- Postoperative precautions: Avoid heavy lifting, maintain blood pressure control and attend regular follow-up visits
- Potential downside: Higher risk of cardiac, respiratory and wound-related complications due to the invasive nature of surgery
Treatment for Ruptured AAA
Ruptured AAA is a vascular emergency requiring immediate surgical treatment.
- Emergency surgery: Either EVAR or open surgical repair is performed urgently, depending on anatomy and patient stability
- Massive internal bleeding: Rapid blood loss can lead to shock, organ failure and death within hours
- Emergency EVAR: Increasingly preferred in suitable patients due to lower short-term mortality
- Haemodynamic stabilisation: Blood transfusions, blood pressure support and ICU monitoring are critical
- Postoperative intensive care: Organ support and close monitoring are often required after rupture repair
Risks & Complications Related to AAA Treatment
AAA repair is highly effective, but like all vascular procedures, it carries certain risks and complications.
- Endoleak after EVAR: Blood continues flowing into the aneurysm sac despite stent graft placement
- Graft complications: Migration, blockage or infection of the graft may occur over time
- Bleeding and clot formation: Possible during or after both EVAR and open surgery
- Kidney injury: Can develop due to contrast exposure or reduced blood flow during procedures
- Cardiac complications: Heart-related complications are more common after open repair
- Respiratory complications: Pneumonia or breathing difficulties may occur after major surgery
- Recurrent aneurysm expansion: Continued enlargement can still increase rupture risk if follow-up is missed
Take Home Message
Abdominal aortic aneurysms often remain silent for years, which is why many patients are diagnosed only after incidental imaging or during emergency rupture. Early screening in high-risk individuals can identify aneurysms before they become life-threatening.
Modern vascular surgery has significantly improved outcomes through minimally invasive procedures like EVAR and advanced open surgical techniques. However, the timing of intervention remains critical because rupture carries extremely high mortality despite emergency treatment.
Long-term success after abdominal aortic aneurysm repair depends on strict follow-up imaging, smoking cessation and cardiovascular risk management. Early vascular consultation can help prevent rupture and improve survival outcomes.
FAQs
Can a ruptured AAA be repaired?
Yes, ruptured AAA can be repaired through emergency vascular surgery, although they remain highly life-threatening conditions. Treatment usually involves emergency EVAR or open surgical repair depending on the patient’s stability and aneurysm anatomy.
Rapid diagnosis and immediate intervention significantly improve survival chances. Delayed treatment increases the risk of severe blood loss, shock, organ failure and death.
How long does ruptured AAA surgery take?
Ruptured AAA surgery generally takes around 2-4 hours, depending on the complexity of the aneurysm, bleeding severity and patient stability. EVAR procedures are often quicker than open surgical repair when anatomically feasible.
Additional time may be required for blood transfusion, haemodynamic stabilisation and postoperative intensive care. Recovery duration varies widely depending on organ function, blood loss and associated complications.
What is the survival rate after AAA repair?
The survival rate after elective abdominal aortic aneurysm repair is generally good when treated before rupture. Studies report a 10-year survival rate of over 70% after planned AAA repair.
Survival is significantly lower in ruptured aneurysms, making early diagnosis and timely treatment critical. Outcomes depend on age, aneurysm size, cardiovascular health and overall medical condition.
How to prevent abdominal aortic aneurysm?
Preventing AAA mainly involves reducing vascular damage and controlling risk factors that weaken the aortic wall.
Stop smoking, control blood pressure, manage cholesterol levels and maintain a healthy body weight.