Snapshot
- Purpose: Dialysis access provides a reliable pathway for blood to flow between the body and the dialysis machine during haemodialysis.
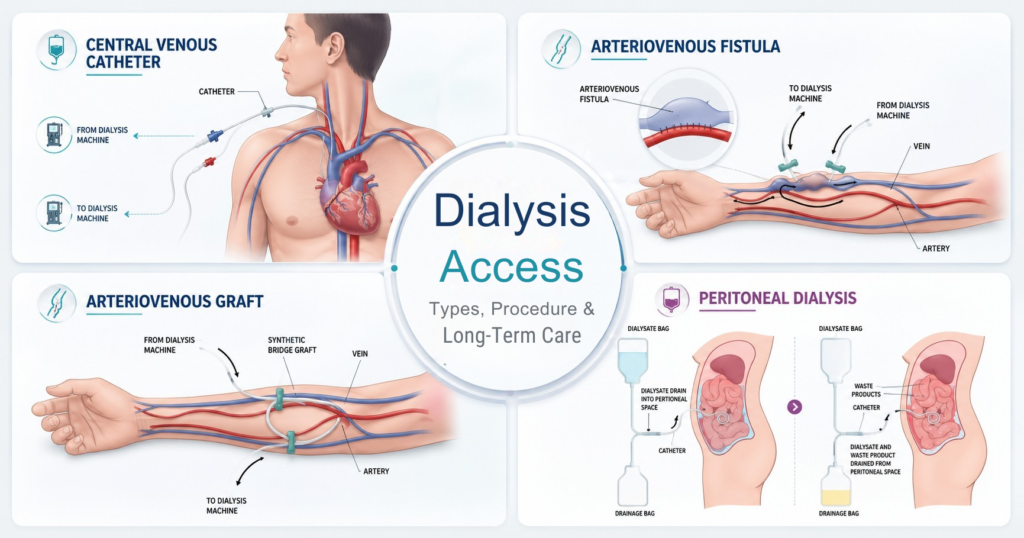
- Dialysis Access Types: AV fistula, AV graft and central venous catheter are the three primary types of vascular access for dialysis.
- Best Dialysis Access: AV fistulas are considered the gold standard due to their longer lifespan and lower risk of infection and clotting.
- Common Complications: Stenosis, thrombosis, infection, aneurysm formation and steal syndrome can affect access function.
- Long-Term Care: Daily access monitoring, proper hygiene and regular vascular surveillance help maintain access patency and dialysis efficiency
Synopsis
Dialysis access is often referred to as the lifeline of haemodialysis because it allows blood to be safely removed, filtered and returned to the body during treatment. The type of access used can significantly influence dialysis effectiveness, complication rates and long-term outcomes.
AV fistulas remain the preferred option for most patients, while AV grafts and catheters may be required in specific situations. Proper access creation, surveillance and maintenance are essential to preserve function and prevent complications that may interrupt dialysis treatmen
What is Dialysis Access?
Dialysis is a life-saving treatment for people with kidney failure. To perform dialysis safely and effectively, a reliable access route is essential. There are two main types of dialysis: haemodialysis and peritoneal dialysis.
Haemodialysis filters blood through a dialysis machine, while peritoneal dialysis uses the peritoneum (the lining of the abdomen) as a natural filter to remove waste and excess fluid. Both methods require stable, long-term access to the body for effective treatment.
In haemodialysis, this access is provided by a vascular access, a surgically created connection between an artery and a vein that allows blood to circulate to and from the dialysis machine. In peritoneal dialysis, a soft catheter is placed in the abdomen to deliver and drain a cleansing fluid called dialysate.
Why Is Dialysis Access Needed?
- Haemodialysis requires steady blood circulation through the dialysis machine.
- Normal veins cannot support high-flow dialysis treatments repeatedly.
- Specialised vascular access provides reliable long-term entry to the bloodstream.
- Well-functioning access reduces treatment interruptions, infections and dialysis-related complications.
What Are the Types of Dialysis Access?
Dialysis access differs depending on the type of dialysis advised. Haemodialysis requires vascular access to the bloodstream, while peritoneal dialysis uses a catheter placed in the abdomen.
The table below compares the common dialysis access options.
| Feature | AV Fistula | AV Graft | Central Venous Catheter | PD Catheter |
| Dialysis Type | Haemodialysis | Haemodialysis | Haemodialysis | Peritoneal Dialysis |
| Longevity | 10+ years | 2-5 years | 1-2 years | Up to 5 years |
| Infection Risk | Lowest | Moderate | Highest | Moderate |
| Clotting Risk | Lowest | Higher | Highest | Not applicable |
| Time Before Use | Weeks to months | 2-4 weeks | Immediate | 2-3 weeks |
| Blood Flow Performance | Best | Good | Lower | Not applicable |
| Preferred For | Long-term haemodialysis | Limited vein options | Urgent haemodialysis | Home-based peritoneal dialysis |
Arteriovenous (AV) Fistula
An AV fistula is created by directly connecting an artery to a vein, usually in the forearm or upper arm. In selected patients with unsuitable arm veins or failed upper-limb access, it may be created in the thigh (femoral region).
This connection increases blood flow through the vein, causing it to enlarge and strengthen over time.
- The most durable and gold standard dialysis access.
- Lowest risk of infection and thrombosis.
- Better long-term patency than other access types.
- Requires maturation before use, often around 4-6 weeks.
Clinical studies support AV fistulas as the gold standard of vascular access, given their association with fewer complications and improved long-term outcomes.
Arteriovenous (AV) Graft
An AV graft uses a synthetic tube to connect an artery and a vein when native veins are unsuitable for fistula creation.
- Suitable for patients with small or damaged veins.
- Can generally be used sooner than a fistula.
- Higher risk of infection and clotting.
- Requires ongoing surveillance to maintain patency.
AV grafts generally require more reinterventions than AV fistulas to maintain long-term patency because they are more prone to narrowing and clot formation.
Central Venous Catheter (CVC)
A central venous catheter is a flexible tube inserted into a large vein, usually in the neck or chest.
- CVC can be used immediately upon insertion.
- Commonly used when urgent dialysis is required.
- Often serves as a temporary solution while a fistula or graft matures.
- Highest risk of infection or thrombus formation and catheter-related complications.
While catheters provide direct access to the bloodstream, they are intended for short-term use and should be replaced with a fistula or graft as soon as feasible.
Peritoneal Dialysis (PD) Catheter
- Soft, flexible catheter permanently placed into the abdominal cavity
- Used for peritoneal dialysis rather than haemodialysis
- Delivers and drains dialysis fluid through the lining of the abdomen (peritoneum)
- Suitable for patients choosing home-based peritoneal dialysis
- Requires regular catheter care to reduce the risk of infection, including peritonitis (infection of abdominal cavity)
Current vascular access guidelines recommend minimising long-term catheter dependence whenever possible because of the increased risk of bloodstream infections and access failure.
How Is Dialysis Access Created?
Creating dialysis access requires careful planning to ensure long-term success and preserve future access options.
Pre-Procedure Evaluation
Before surgery, vascular specialists assess the arteries and veins to determine the most suitable type of access.
- Vein mapping on ultrasound evaluates vessel size, location, depth, and tortuous course.
- Medical history and vascular health are reviewed.
- Access planning helps prevent dialysis complications.

Pre-operative vessel screening has improved fistula success rates and remains a standard component of access planning.
Access Creation Procedure
Most access procedures are performed as day-care surgeries under local or regional anaesthesia.
- Access location depends on vascular anatomy.
- Surgeons generally prioritise the non-dominant arm.
- Future dialysis requirements are considered during planning.
Access Maturation
Following surgery, the access must develop adequate blood flow before routine dialysis can begin.
- Veins enlarge and strengthen after fistula creation.
- Blood flow gradually increases during maturation.
- Regular monitoring helps identify early maturation failure.
Early intervention for non-maturing fistulas can improve long-term access success and reduce catheter dependence.
Common Complications of Dialysis Access
Although modern vascular access techniques are highly effective, complications can still occur.
- Access stenosis: Narrowing of the access reduces blood flow and is one of the most common causes of dysfunction.
- Thrombosis: Blood clot formation can suddenly block the access and often develops secondary to untreated stenosis.
- Infection: Particularly common with catheters and may progress to serious bloodstream infections.
- Aneurysm formation: Repeated needle punctures can weaken the vessel wall and cause abnormal bulging.
- Steal syndrome: Excessive diversion of blood into the access may reduce circulation to the hand, causing pain, numbness or finger discolouration.
- Access failure: Severe narrowing, clotting or recurrent complications may ultimately result in loss of access function.
Access dysfunction, including narrowing (stenosis), clotting (thrombosis) or inadequate blood flow, is a major cause of hospitalisation and intervention among haemodialysis patients. Regular surveillance helps detect these problems early.
Vascular Access Maintenance Tips
Daily self-care, access monitoring and regular follow-up help maintain adequate blood flow and detect problems before they affect dialysis.
- Keep the access site clean and dry, especially during the healing period.
- Perform hand-grip exercises after AV fistula surgery, if advised, to support fistula maturation.
- Avoid lifting heavy weights or sleeping on the access arm.
- Do not wear tight clothing, jewellery or blood pressure cuffs on the access arm.
- Check for the characteristic vibration (“thrill”) every day if you have an AV fistula or graft.
- Report swelling, redness, pain, prolonged bleeding or loss of thrill promptly.
- Attend scheduled follow-up visits to assess healing, blood flow and early signs of narrowing or access dysfunction.
Patient education plays a critical role in maintaining patency of access and preventing avoidable complications.
Take Home Message
Choosing the right dialysis access is essential for safe and effective long-term dialysis. AV fistulas are the preferred option for most patients, but the best access depends on your vascular health, dialysis needs and overall medical condition.
Creating dialysis access is only the beginning. Regular monitoring, proper access care and early treatment of problems such as narrowing, clotting or infection help preserve access function and reduce treatment interruptions. Close follow-up with your nephrologist and vascular specialist supports better long-term dialysis outcomes.
FAQs
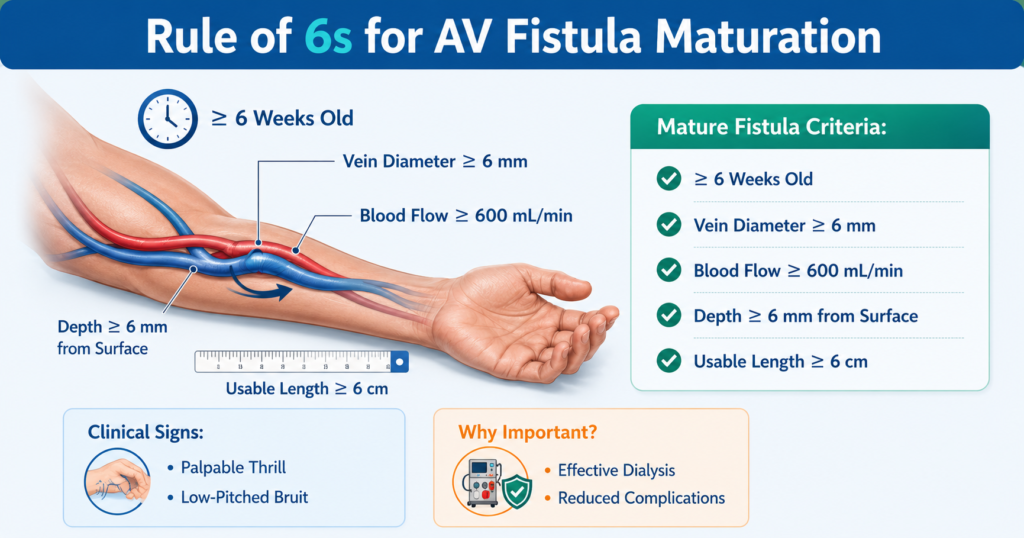
What Is the Rule of 6 for Dialysis Access?
The rule of 6 is commonly used to assess AV fistula maturation before dialysis use. A mature fistula should generally have a vein diameter of at least 6 mm, blood flow greater than 600 mL/min and a depth of less than 6 mm beneath the skin surface. These measurements help ensure successful needle cannulation and effective dialysis treatment.
What Is Access Recirculation in Dialysis?
Access recirculation occurs when purified blood returning from the dialysis machine re-enters the dialysis circuit instead of circulating through the body. This reduces dialysis efficiency and may indicate access stenosis, inadequate blood flow or incorrect needle placement. Identifying and correcting the underlying issue is important to maintain treatment adequacy.
What are the Signs of Hemodialysis Access Failure?
Common warning signs include loss of the normal thrill or bruit at the access site, arm swelling, pain, prolonged bleeding after dialysis and difficulty achieving adequate dialysis blood flow. These symptoms may indicate narrowing, clotting or other access-related complications and should be evaluated promptly by a vascular specialist.